Alexander Ahammer, Stefan Bauernschuster, Martin Halla, Hannah Lachenmaier 27 March 2021
Europe leads the world in alcohol consumption. According to WHO, more than 10.3 million disability-adjusted life years were lost due to alcohol abuse in 2016, and 10% of all deaths are attributable to alcohol (World Health Organization 2018). Teenage binge drinking is much more prevalent in Europe than in the US, a disparity often attributed to the large difference in minimum legal drinking ages (MLDAs). While US teenagers are prohibited from drinking alcohol before turning 21, the MLDA in most European countries is 18. Some countries even allow drinking for teenagers as young as 16. Proponents of low MLDAs suggest that they foster more responsible alcohol consumption later in life, while critics argue that youth drinking may have detrimental effects on brain development.
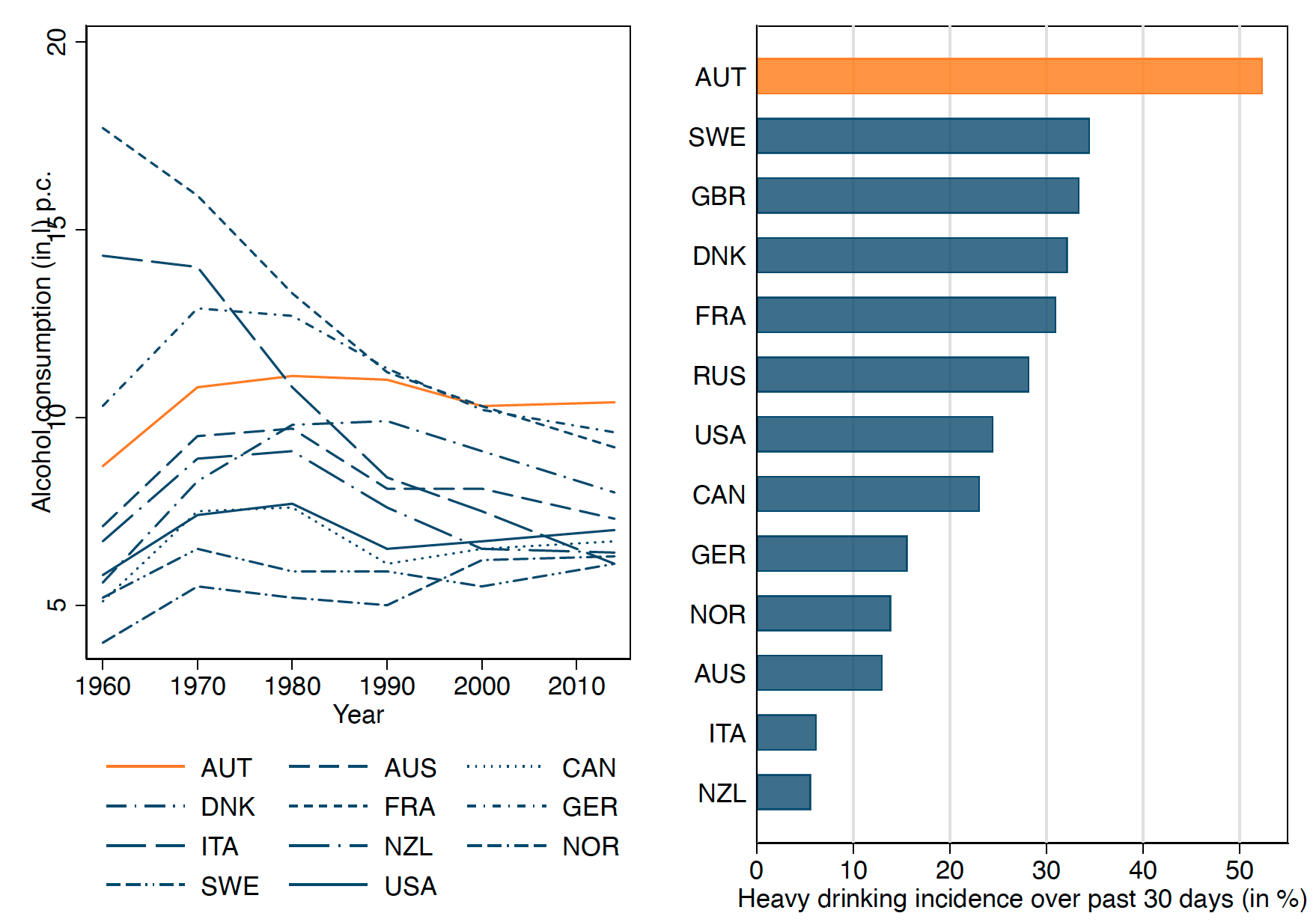
There is a large literature on the effects of the MLDA on a variety of outcomes, such as alcohol and drug use (e.g. Carpenter Dobkin Warman 2016, Crost and Rees 2013), mortality (e.g. Carpenter and Dobkin 2009), crime (e.g. Carpenter and Dobkin 2015), drinking and driving (e.g. Miron and Tetelbaum 2007), and schooling (e.g. Lindo et al. 2013). Most of these studies are based on US or Canadian data, where the MLDA is high. We complement this literature by studying teenage binge drinking in Austria, which has an MLDA of 16 years (Ahammer et al. 2021). Austria is particularly interesting because it is among the countries with the highest levels of alcohol consumption worldwide (see Figure 1). Moreover, we can draw from an excellent data pool in Austria. We use both high-quality survey data and administrative health registers, which allow us to take a closer look at the socioeconomic gradient in binge drinking and the mechanisms behind MLDA legislation.
Figure 1 Alcohol consumption: International comparison
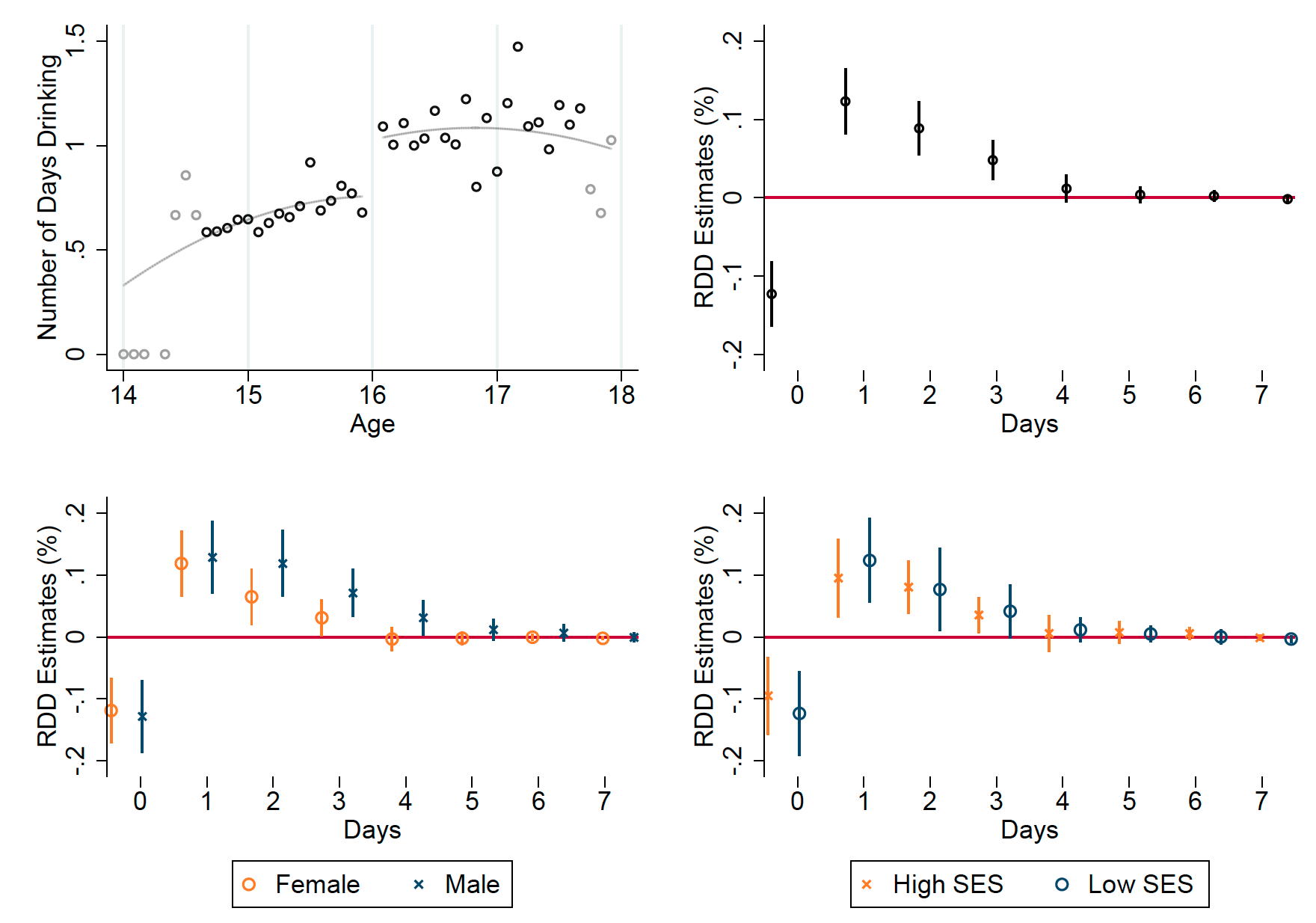
First, we want to know how drinking behaviour changes as teenagers age across the MLDA threshold. To this end, we pull data on self-reported alcohol consumption in Austria from the European School Survey Project on Alcohol and Other Drugs (ESPAD). We compare teenagers who were just above and just below 16 years of age when taking the survey and find a clear discontinuous increase in past-week drinking at age 16, which – according to our regression discontinuity (RD) models – amounts to roughly 0.3 days (see Figure 2). The probability of drinking at least once in the past week increases by 12 percentage points at age 16. We also find interesting heterogeneities by sex and socioeconomic status. Male and low socioeconomic status (SES) teenagers tend to increase heavy drinking more than young women when alcohol becomes legally available.
Figure 2 Effect on number of days drinking during the last seven days
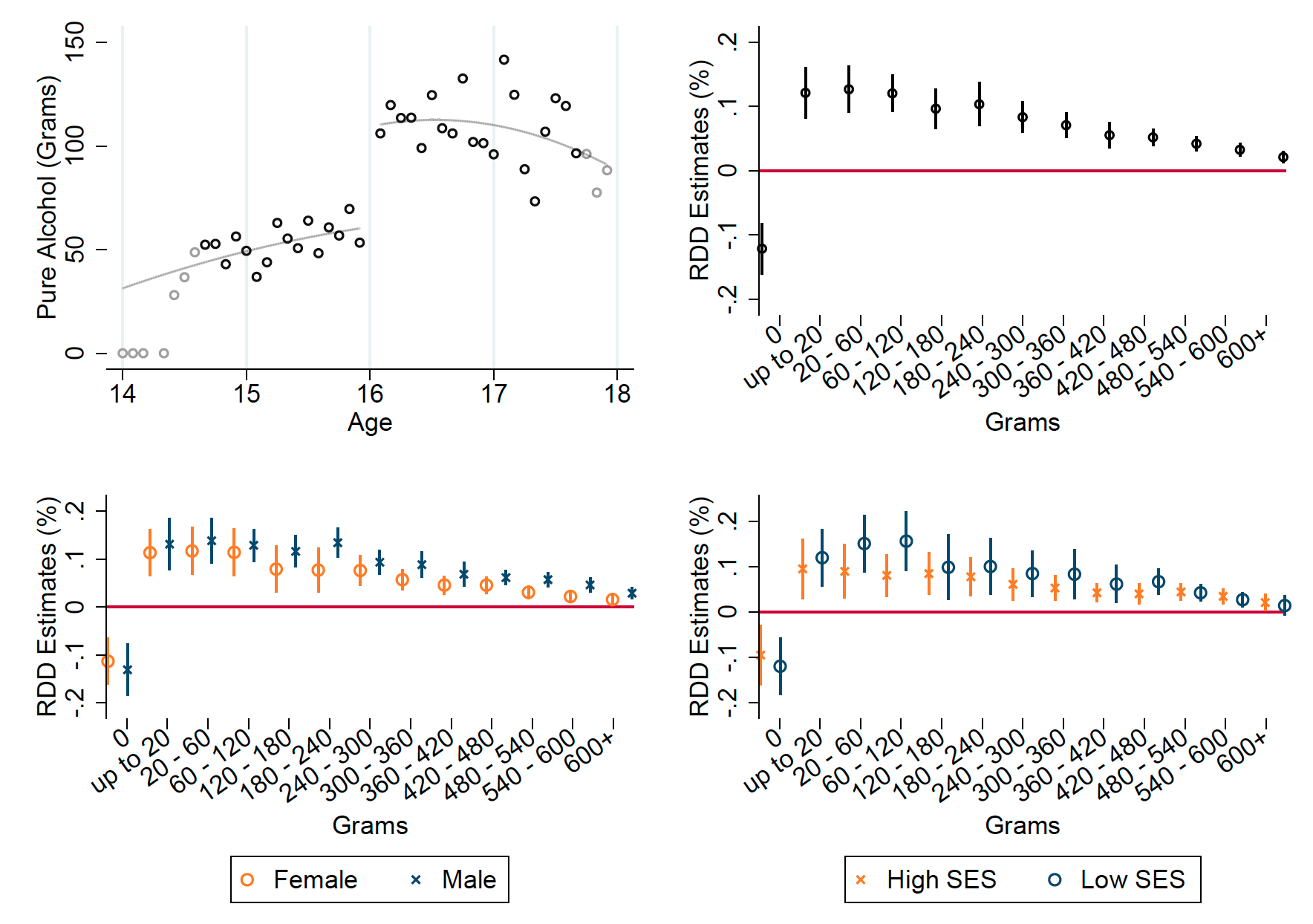
The ESPAD also has information on the quantity of alcohol consumed. Again, there is a noticeable jump at age 16, amounting to about 50 more grammes of pure alcohol consumed in the past week (Figure 3). This is almost double the pre-16 level. These positive effects appear along the full drinking distribution. The probability that teenagers consume at least 180–240 grammes more – equivalent to an extra 9–12 pints of beer – increases by 10 percentage points too. As before, we find that male and low-SES teenagers are more likely to drink excessive amounts.
Figure 3 Effects on grammes of pure alcohol consumed during the last seven days
In a next step, we want to know how these changes in drinking behaviour translate to morbidity. This is important, because the societal cost of drinking alcohol likely skyrockets once it leads to hospitalisation, especially with teenagers. Using high-quality administrative health records from the Upper Austrian Health Insurance Fund (UAHIF), we pull information on hospitalisations due to alcohol poisoning for the full population of children born between 1991 and 1995 in Upper Austria. Alcohol poisonings are a rather rare outcome (one in a thousand children in our data suffer from alcohol poisoning), but the advantage of these data is that we do not have to worry about reporting problems or recall bias.
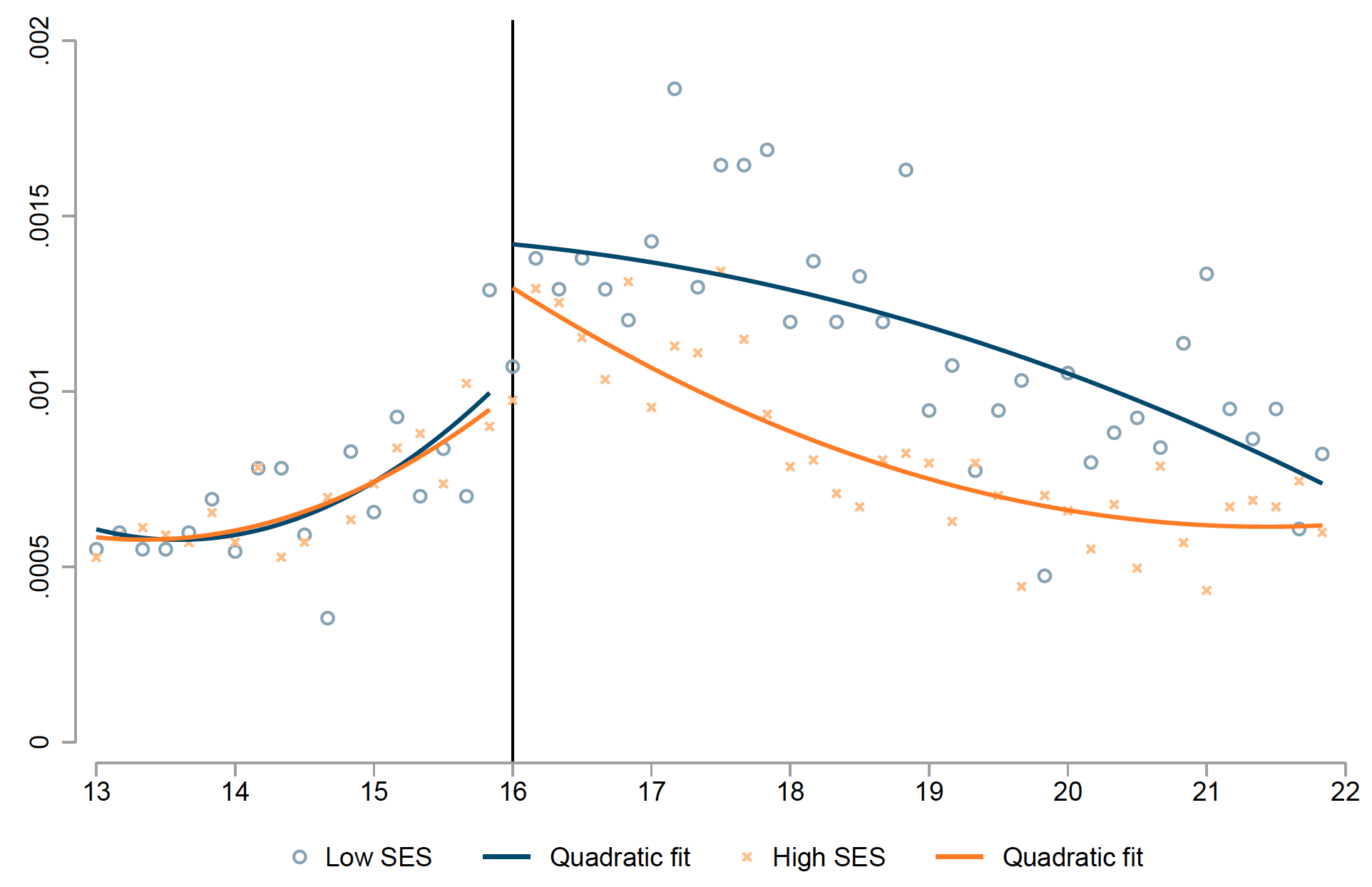
When we look at the probability that a teenager is admitted to hospital with alcohol poisoning by age, we find a very similar jump at the MLDA threshold. The discontinuity estimate suggests a 42% increase at age 16 (Figure 4). Splitting by SES reveals an interesting pattern. The age trends in poisonings are almost overlapping before age 16, but low SES teenagers seem to respond more strongly at the MLDA cutoff. We then see that poisonings are a concave function of age for low SES, but a convex function for high SES teenagers. The resulting socioeconomic gap is largest between ages 17 and 18, after which it converges. Even at age 22, there is still a statistically significant difference in poisonings between low- and high-SES teenagers.
Figure 4a Probability of being hospitalised with an alcohol intoxication
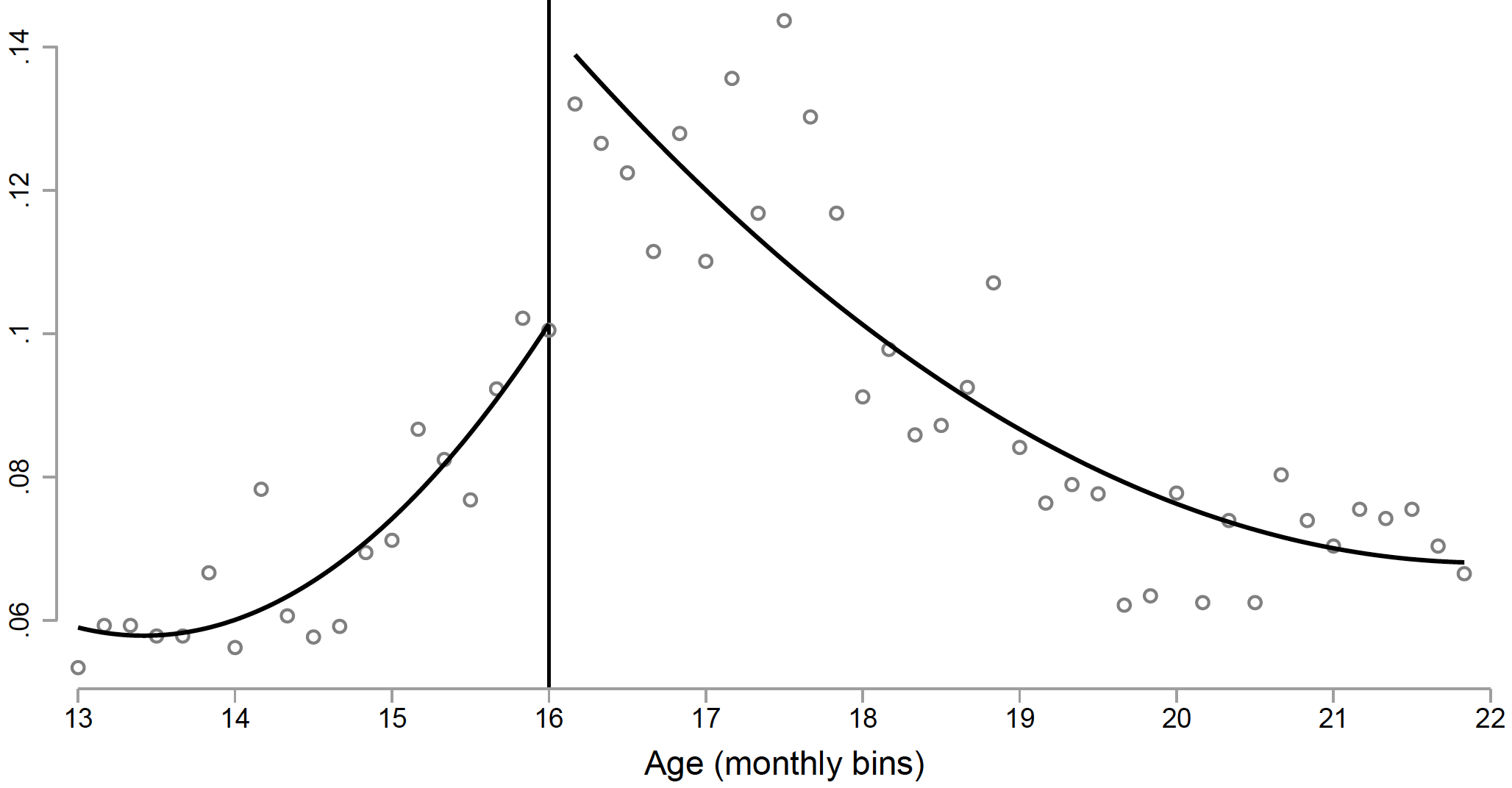
Figure 4b Probability of being hospitalised with an alcohol intoxication by socioeconomic status
Another advantage of our register data is that we can investigate whether teenagers that are exposed to alcohol abuse in the family react differently to MLDA regulation. To this end, we identify teens whose parents were diagnosed with alcohol-induced liver cirrhosis. Interestingly, it seems that these teenagers do not change their behaviour at age 16. One might be tempted to interpret this as a deterrence effect, but given that the incidence of alcohol poisonings is much higher in families with a history of alcohol abuse, we interpret this as a sign that teenagers imitate their parents’ behaviour and engage more often in excessive drinking, regardless of whether they are legally allowed to drink. In high-risk groups, therefore, MLDA may not be effective.
What drives this sharp increase in alcohol abuse at age 16? We have two mechanisms in mind: access and risk perceptions. To gauge the importance of access, we first use new data from a mystery shopping study in Upper Austria, where underage test buyers visit retail shops and attempt to purchase liquor. Out of 4,269 purchase attempts, around 23% were successful. Hence, only three-quarters of retailers comply with MLDA regulation, which may point to an enforcement problem. If we aggregate these attempts at the municipal level and merge socioeconomic information, we find that the socioeconomic composition does not correlate with retailer compliance. This is in line with the observation that, prior to age 16, there is no difference in binge drinking between children from different socioeconomic backgrounds. Also in the ESPAD survey, 84% of 15 year-olds perceive access to alcohol as ‘easy’ or ‘rather easy’. Taken together, these findings suggest that a lack of access to alcohol can hardly explain the effectiveness of MLDA legislation.
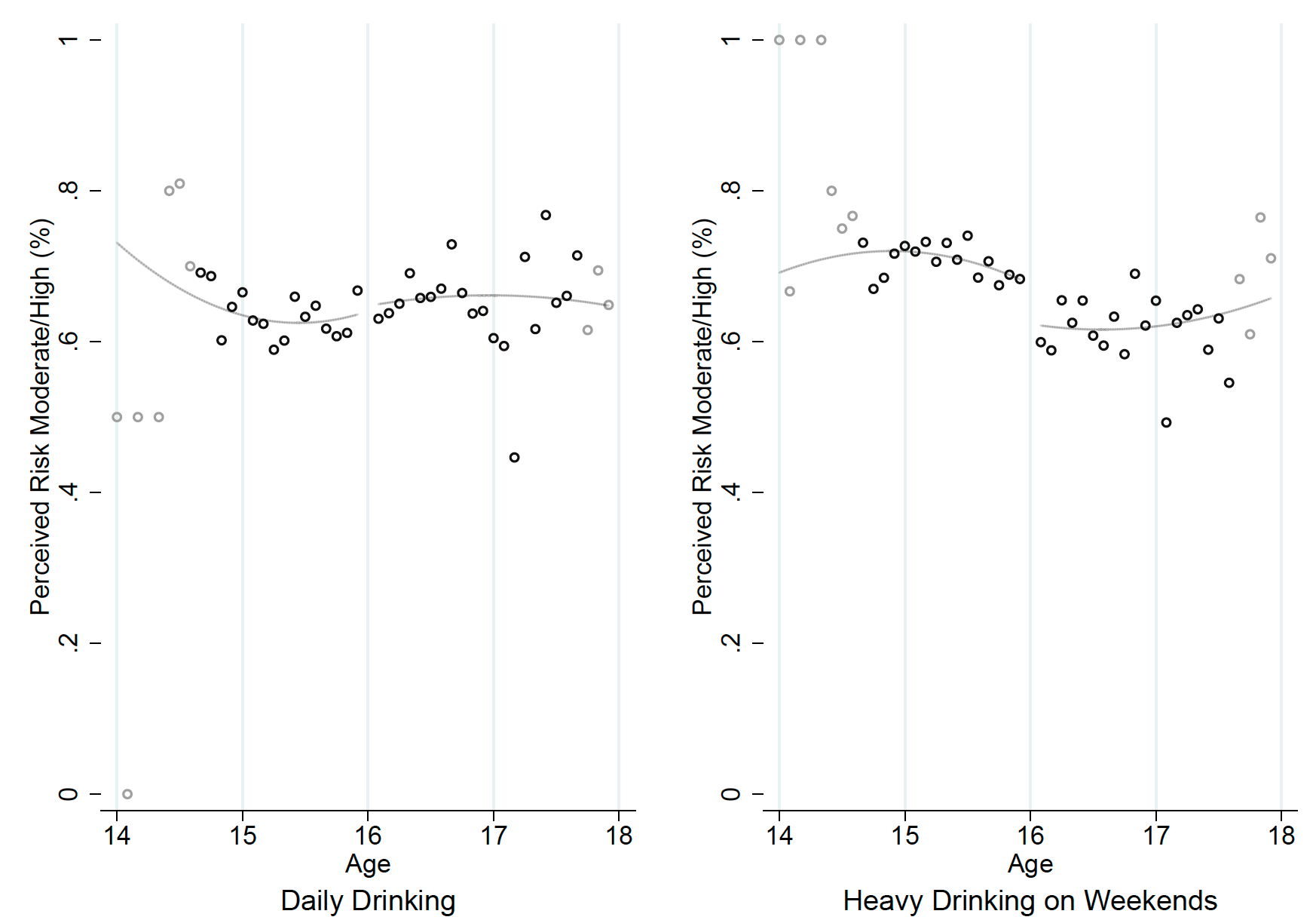
A plausible complementary mechanism is that MLDA legislation has established a normative value, in the sense that some teenagers simply feel obliged to obey and abstain from drinking alcohol before age 16, despite its availability. In addition, parents may become more lenient when their child reaches age 16 and drinking becomes not just legally allowed, but also socially accepted. This normative mechanism is difficult to test empirically. The ESPAD survey, however, includes a question on risk perceptions about alcohol, which we can use as a surrogate outcome. Absent MLDA legislation, we expect risk perceptions to be a continuous function of age, but this is not what we see in the data. In fact, the perceived risk of heavy drinking during weekends decreases significantly at the MLDA cutoff (Figure 5). We interpret this as suggestive evidence for a normative impact of the legislation.
Figure 5 Risk perception of daily drinking and heavy drinking at weekends
To conclude, we find that teenagers increase both the frequency and the intensity of drinking at the MLDA cutoff, and these effects tend to be stronger for boys and low SES teenagers. We show that these effects persist for some years and cannot be explained by birthday effects. We also find some evidence that a normative effect of the legislation, and not access to alcohol, might explain the MLDA effect.
Unfortunately, we cannot perform a comprehensive welfare analysis. However, if we are worried about SES disparities, our results suggest that a (stepwise) increase of the MLDA would reduce the number of alcohol poisonings and the early socioeconomic gradient in teenage binge drinking. As an alternative to raising the MLDA for everybody, it might be worth considering measures that particularly target teenagers with a low socioeconomic background to avoid an early socioeconomic gradient in harmful binge drinking. This might also be the preferred option for teenagers from families with a history of severe alcohol abuse, since MLDA regulations are not effective for this high-risk group. Moreover, targeted measures in high-risk geographical areas may be useful (Hinnosaar and Liu 2020).
References
Ahammer, A, S Bauernschuster, M Halla and H Lachenmaier (2021), “Minimum Legal Drinking Age and the Social Gradient in Binge Drinking”. IZA Discussion Paper No. 13987.
Carpenter, C and C Dobkin (2009), “The Effect of Alcohol Consumption on Mortality: Regression Discontinuity Evidence from the Minimum Drinking Age”, American Economic Journal: Applied Economics 1(1): 164–182.
Carpenter, C and C Dobkin (2015), “The Minimum Legal Drinking Age and Crime”, Review of Economics and Statistics 98(2): 254–267.
Carpenter, C, C Dobkin and C Warman (2016), “The Mechanisms of Alcohol Control”, Journal of Human Resources 51(2): 328–356.
Crost, B and D I Rees (2013), “The Minimum Legal Drinking Age and Marijuana Use: New Estimates from the NLSY97”, Journal of Health Economics 32(2): 474–476.
Hinnosaar, M and E Liu (2020), “Malleability of alcohol consumption”, VoxEU.org, 18 October.
Lindo, J M, I D Swensen and G R Waddell (2013), “Alcohol and Student Performance: Estimating the Effect of Legal Access”, Journal of Health Economics 32(1): 22–32.
Miron, J and E Tetelbaum (2007), “What Europe can learn from US policies on drinking and driving”, VoxEU.org, 5 September.
World Health Organization (2018), Adolescent Alcohol-Related Behaviours: Trends and Inequalities in the WHO European Region, 2002-2014.
World Health Organization (2019), Status Report on Alcohol Consumption, Harm and Policy Responses in 30 European Countries 2019.
"social" - Google News
March 27, 2021 at 07:04AM
https://ift.tt/2PAOZIN
Minimum legal drinking age and the social gradient in binge drinking | VOX, CEPR Policy Portal - voxeu.org
"social" - Google News
https://ift.tt/38fmaXp
https://ift.tt/2WhuDnP
Bagikan Berita Ini














0 Response to "Minimum legal drinking age and the social gradient in binge drinking | VOX, CEPR Policy Portal - voxeu.org"
Post a Comment