Vaccine availability does not necessarily entail widespread vaccination demand, as a share of the population may be unwilling to be vaccinated. The World Health Organization (WHO) declared vaccine hesitancy as one of the top ten global health threats in 2019, and vaccine hesitancy and acceptability mean the perceived social value of a vaccine is variable. Yet, the uptake of vaccines is often challenged by individuals and groups who refuse to be vaccinated on religious, philosophical, or socio-political grounds (Wolfe and Sharp 2002) and can be influenced by how strained emergency healthcare services were during the first wave of the pandemic (Blanchard-Rohner et al. 2021). As a result, a population’s perception of the social value of a vaccine depends, in part, on individual preferences. What are the social and individual estimates of the social value of a Covid-19 vaccine, and how can we incentivise vaccine uptake?
The social value of a vaccine
The social value of a vaccine exceeds its private value, given the ‘protective effects’ for the wider population. Indeed, vaccines exert large positive externalities on others in society, including the unvaccinated. For instance, in terms of health security, vaccine take-up increases the probability of a community reaching herd immunity (i.e. point at which a proportion of the population is immune to a disease), which has direct impacts on others by reducing contagion, preventing morbidity and mortality, and diminishing the need for restrictions that hamper economic activity and social life.
Estimating the value of a vaccine to individuals and society is affected by individual perception on multiple levels (e.g. the vaccine itself, the development process, regulatory agencies). Using evidence of stock prices and a novel vaccine progress indicator, some studies have estimated the value of a Covid-19 cure to be about 5–15% of total global wealth (Acharya 2021).
In a new paper (Costa-Font et al. 2021), we elicit willingness to pay (WTP) for a hypothetical vaccine during the first wave of the Covid-19 pandemic in four western countries (the US, the UK, Spain, and Italy). By using a payment card method, we estimate a monetary equivalent value of a SARS-CoV-2 vaccine (compensating variation) independently of its efficacy and characteristics.
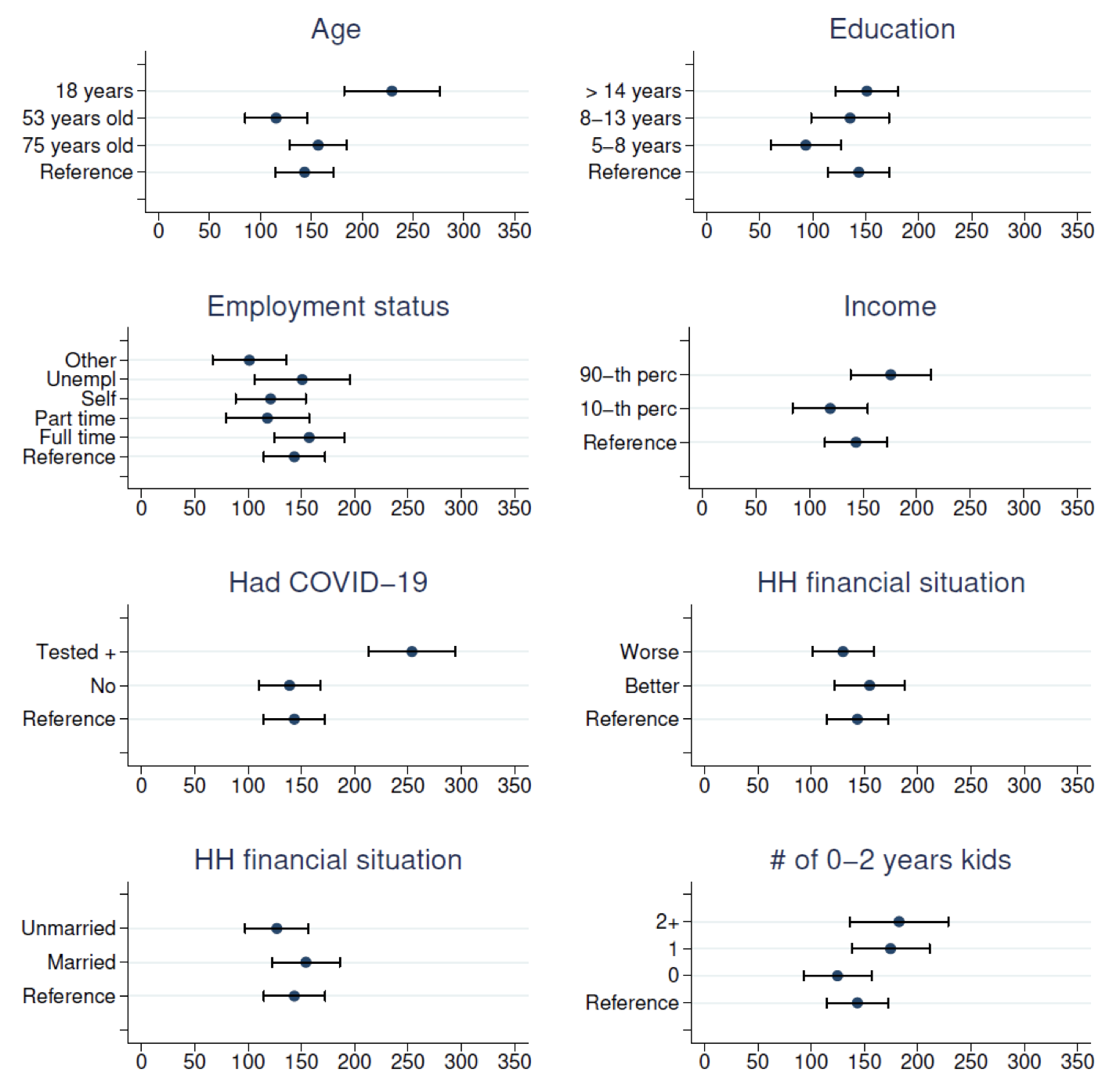
Our estimates suggest that the social value of such a vaccine exceeds its market value. The willingness to pay estimates are elicited using a payment card method to avoid ‘yea saying’ biases, and we study the effect of protest response, sample selection bias, as well as the influence of trust in government and risk exposure. We find the average value of a hypothetical vaccine to be US$100-200 (once adjusted by purchasing power) in a sample of the four western countries. Findings demonstrate no variation between Spain and Italy but are higher in the UK and lower in the US. Our results reveal that the willingness to pay in the US results, in part, from respondents’ mistrust in the national government – respondents who trust the US government declare a willingness to pay equal to respondents in the other countries. Figure 1 reveals a higher willingness to pay by younger and more affluent individuals, those who had Covid-19, and those who have children. Willingness to pay estimates are lower in the US than in most European countries.
Figure 1 Corelates of willingness to pay for a COVID-19 vaccine ($)

Incentivising vaccine uptake
Vaccine uptake might not necessarily come from a self-protective motive, but from pro-social behaviour to protect the wider community. By this logic, risk-seeking and less pro-social individuals (Betsch et al. 2013) are less likely to vaccinate. But what we know from motivating pro-social behaviours in health care (Costa-Font and Machado 2021) is that they are very sensitive to small incentives and the lifting of constraints, and this is especially the case when it comes to vaccines (Beshears et al. 2016). Madrian (2014) considers the case of a subsidy with other behavioural interventions that nudge individuals to get vaccinated, so that the marginal social value of the vaccine moves closer to the private social value. Yet, she argues that there would always be individuals that might be vaccine-hesitant and sensitive to subsidies that change the marginal costs of taking up the vaccine. Subsidies can therefore backfire if people perceive subsidised actions as entailing risks to be compensated for. At present, the US offers a long list of examples of how to incentivise vaccine uptake, even including free beers.
Other alternatives include making vaccination compulsory. But, as with compulsory voting, the administrative costs to operationalise compulsory vaccination (and fines for those failing to comply) might be counterproductive and can feed further antagonism and resistance (let alone conspiracy theories of those arguing the government wants to use vaccination as a form of social control). A less intrusive form of intervention is to condition access to non-essential activities on getting the jab. But this can be discriminatory until everyone has at least had the chance to get the vaccine (and will need a list of exclusions). And again, it might not help build a positive narrative about the pro-social effect of vaccination.
An alternative lies in using nudges and reducing constraints to getting the vaccine, such as vaccination default times or piggybacking on other activities such as vaccination socials. Social incentives can be enacted by changing or improving the social esteem of those who get vaccinated without stigmatising those who decide not to, thereby creating desirable network effects. Changing the narratives of vaccination so individuals that refuse to be vaccinated understand that the default option is to get vaccinated can make a difference. The role of celebrities taking up vaccines and promoting them is also important.
Finally, one of the main issues with vaccine uptake is proper knowledge of how vaccines benefit both individuals and society, and convincing people they should be able to control the potential side effects of a jab. Vulnerability to fake news and access to sceptical social media can lead people to overestimate rare side effects and ignore the small probability of occurrence (which is labelled as ‘erring on the side of rare events’). Traditional risk awareness can make a difference. Media groups have a responsibility to play down and not to amplify the small risks associated with vaccination and have the power to portray a positive representation of the benefits of vaccinations and the negligible nature if its risks. This might involve other societal stakeholders such as community and local leaders or trade unions, who can support public health authorities and medical profession such as GPs.
Covid-19 vaccines exert large positive spillover effects beyond their protective effects for individuals. The value of vaccines therefore far exceeds their costs, or even their private benefit. But in shaping behaviour, incentives need to be more nuanced, and traditional incentives (such as subsidies) are unlikely to work. This seems to be fertile ground for the ‘nudge’ agenda and for the design of wider social incentives that boost the social esteem of those who get vaccinated.
References
Acharya, V (2021), “The value of a cure for COVID-19: What are asset prices telling us?”, VoxEU.org.
Blasi, F, S Aliberti, M Mantero and S Centanni (2012), “Compliance with anti-h1n1 vaccine among healthcare workers and general population”, Clinical Microbiology and Infection 18(5): 37–41.
Beshears, J, J J Choi, D I Laibson, B C Madrian and G I Reynolds (2016), “Vaccination rates are associated with functional proximity but not base proximity of vaccination clinics”, Medical Care 54(6): 578.
Betsch, C, R Bohm and L Korn (2013), “Inviting free-riders or appealing to prosocial behavior? Game-theoretical reflections on communicating herd immunity in vaccine advocacy”, Health Psychology 32(9): 978–985.
Blanchard-Rohner, G, B Caprettini, D Rohner, H-J Voth (2021), “From tragedy to hesitancy: How public health failures boosted COVID-19 vaccine scepticism”, VoxEU.org, 01 June.
Costa-Font, J, C Rudisill, S Harrison and L Salmasi (2021), “The Social Value of a SARS-CoV-2 Vaccine: Willingness to Pay Estimates from Four Western Countries”, IZA Working Paper 14475.
Costa-Font, J and S Machado (2021), “How can policy interventions encourage pro-social behaviours in the health system?”, LSE Public Policy Review 1(3).
Madrian, B C (2014), “Applying insights from behavioral economics to policy design”, Annual Review of Economics 6(1): 663-688.
Thomson, A, K Robinson and G Vall´ee-Tourangeau (2016), “The 5as: A practical taxonomy for the determinants of vaccine uptake”, Vaccine 34(8): 1018–1024.
"social" - Google News
June 29, 2021 at 06:04AM
https://ift.tt/3jpmnzs
Social value and incentives for vaccine uptake | VOX, CEPR Policy Portal - voxeu.org
"social" - Google News
https://ift.tt/38fmaXp
https://ift.tt/2WhuDnP
Bagikan Berita Ini














0 Response to "Social value and incentives for vaccine uptake | VOX, CEPR Policy Portal - voxeu.org"
Post a Comment